
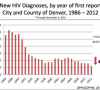
By Katie Kerwin McCrimmon AIDS killed scores of David Lipsons close friends, an adored partner and even his own brother. One of the first men in the nation to be tested for HIV back in 1984, David Lipson received the same terrible test results that ensnared so many of his friends. Then 26 and living in Los Angeles, Lipson learned he was HIV positive and his doctor told him he would die within two years. HIV infection rates are down 45 percent in Denver from 2005. Rates could decrease further if more men engaged in safe sex. Source: Dr. Mark…


