
By Katie Kerwin McCrimmon Drug possession will not be reduced to a misdemeanor in Colorado this year after opposition from prosecutors torpedoed a sentencing reform bill. Instead Senate Bill 12-163 will now require a comprehensive study of Colorados drug sentencing guidelines that could result in new legislation next year. Revisions to the bill are expected to be presented to the Senate Appropriations Committee on Friday. The new bill calls for the drug policy task force of the Colorado Commission on Criminal and Juvenile Justice to convene a study and produce draft legislation within six months. A bipartisan group of lawmakers…
Monthly Archives: April 2012
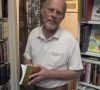
By Katie Kerwin McCrimmon Justin Swanstrom used to be set for life. The 56-year-old Denver lawyer and his partner owned a loft in the trendy Ballpark neighborhood downtown. And Swanstrom had a rental home that provided extra income. Then, last January, he lost his job and two months later, had a heart attack that landed him in St. Joseph Hospital with massive bills and no health insurance. “I received excellent care. I just feel guilty that I couldn’t pay them,” Swanstrom said. He and his partner had to sell the loft. Swanstrom lost the rental to foreclosure. And, he’s subsisting…
By Katie Kerwin McCrimmon Circumcisions for low-income babies could once again be covered in Colorado after a bill seeking to restore funding moved forward Tuesday in the Senate. Circumcision has become a polarizing issue in Colorado after the legislature last year voted to make Colorado the 18th state to ban Medicaid funding for the procedure. The state stopped paying for routine circumcisions last July. Cost is not the primary point of contention. Circumcisions which cost about $200 to $400 each for low-income babies add up to a relatively small tab according to state fiscal analysts: about $195,000 next year and…

By Katie Kerwin McCrimmon Good health makes us happy and happiness makes us healthy. So what are the secrets to becoming happier and healthier? Daniel Gilbert, a Harvard psychologist and author of the bestseller, Stumbling on Happiness, shared his insights on Monday during a speech at his alma mater, the University of Colorado Denver.. His prescription for a happy life could be summed up with these mini-mantras: Get married. Earn at least $50 K. Have sex. Skip kids. Work. Dont try to predict happiness youll be wrong. Women: talk and eat with friends. (Ahh. Happiness is summing up happiness in…
By Katie Kerwin McCrimmon Colorado has made substantial progress in implementing a health insurance exchange, but significant work remains in part because of Colorados flawed computer systems, a new reportfrom the Urban Institute has found. The biggest challenge for Colorado may be that the state is starting with a flawed foundation, a legacy computer system CBMS (Colorado Benefits Management System) that is inflexible and difficult to modify, the report states. Researchers from the Urban Institute are conducting a comprehensive monitoring and tracking project to assess implementation of the Affordable Care Act throughout the U.S. The Robert Wood Johnson Foundation is…
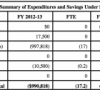
By Katie Kerwin McCrimmon Despite vehement opposition from prosecutors and sheriffs, a bill that would reduce possession of small amounts of drugs from felony offenses to misdemeanors advanced in the Colorado legislature this week. Denver District Attorney Mitch Morrissey told members of the Senate Finance Committee on Tuesday that SB12-163 would destroy Denver’s drug court and undermine his ability to entice addicts into drug treatment because he could no longer threaten them with felonies. A representative for Colorado sheriffs also questioned the costs of the bill. The fiscal note predicts that it will save the state nearly $1 million next year and $2.2 million…

By Katie Kerwin McCrimmon Donations for breast cancer took at hit in Colorado last year and the public battle between national Komen leaders and Planned Parenthood could further reduce fundraising this year, leaving breast cancer survivors without critical help. Already groups like Sense of Security, a small Denver nonprofit that serves low-income breast cancer patients throughout Colorado, have lost thousands of dollars. Sense of Security did not receive funding this year from the Denver affiliate of Susan G. Komen for the Cure, leaving a $60,000 gap in its $400,000 annual budget. Another nonprofit, Rocky Mountain Cancer Assistance, lost $70,000 of its $425,000 annual budget…
By State Rep. Cherylin Peniston These “personhood” zealots will not give up. Not once but twice Colorado voters have overwhelmingly rejected proposed constitutional amendments that would confer “personhood” rights on fetuses. But instead of respecting what the voters have said, Rep. Janak Joshi, R-Colorado Springs, is trying to circumvent the will of the people and impose “personhood” by legislation. House Bill 12-1130, sponsored by Rep. Joshi, would create a new class of crime victim – “an unborn member of the species homo sapiens.” In an essay posted in this space, Rep. Joshi claims it “does not confer the status of ‘person’ upon…
By Katie Kerwin McCrimmon One of the biggest myths about the obesity epidemic is that Americans cant afford fresh fruits and vegetables, Assistant Secretary of Agriculture Kathleen Merrigan said during a visit to Colorado this week. We have 18 million kids in this country who are food insecure while we also have an obesity epidemic, Merrigan said during a talk at the University of Colorado Denver on Thursday. I like to do some myth-busting, she said. People say if we increase the number of fruits and vegetables, it increases the cost. Fruits and vegetables are too expensive. We have a…
By State Rep. Janak Joshi District attorneys and law enforcement officials have repeatedly requested legislation to fix a glaring loophole in Colorado’s criminal justice system. By not creating a separate crime for the death of a pregnant woman’s child through a criminal act, Colorado law fails to protect the rights of pregnant women and their children. To correct this failure in our criminal justice system, I’m sponsoring House Bill 1130. This bill will allow prosecution for a criminal act that results in the death of a pregnant woman’s child. Similar legislation has already been passed in 34 states, including California,…